Erectile dysfunction is one of the most common health concerns affecting men over 40, and one of the least talked about honestly in a clinical setting. Most men who deal with it get offered a prescription and sent on their way without anyone taking the time to figure out what is actually causing the problem.
That approach matters because ED is almost always a symptom, not a disease in itself. It is the downstream signal of something else going on in the body, whether vascular, hormonal, metabolic, neurological, or psychological, and treating the symptom without identifying the cause is what keeps so many men cycling through solutions that work partially, temporarily, or not at all.
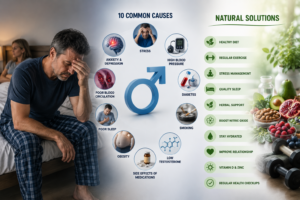
Here are the 10 most common root causes of ED, what is happening biologically in each case, and what natural solutions are available when the cause is properly identified.
What Nobody Tells You About the Real Reasons ED Develops
Understanding the 10 causes of erectile dysfunction requires first understanding what an erection actually needs to happen. It requires a healthy desire signal from the brain, intact nerve pathways carrying that signal, adequate arterial blood flow into penile tissue, healthy smooth muscle that can relax and fill with blood, sufficient testosterone to maintain sensitivity at every level of that chain, and a psychological state that is not actively working against the whole process.
Every one of the causes below disrupts one or more of these requirements. Identifying which one or which combination applies to your situation is what determines which solution actually works for you.
Cause 1: Poor Blood Flow and Vascular Disease

Why the Arteries Feeding Erectile Tissue Are the First to Show Cardiovascular Damage
Vascular disease is the most common underlying cause of ED in men over 40, accounting for the majority of cases that do not have a predominantly psychological explanation. The penile arteries are among the smallest in the body, and small arteries are the first to show the effects of endothelial damage, atherosclerosis, and reduced nitric oxide availability that come with chronic cardiovascular risk factors. This is actually why ED is now considered a significant cardiovascular warning sign. Men who develop vascular ED are statistically at elevated risk for a cardiac event within five to ten years if the underlying vascular disease goes unaddressed.
Nitric oxide is the molecule responsible for relaxing smooth muscle in blood vessel walls and allowing the blood flow surge that produces an erection. When endothelial health deteriorates, nitric oxide production decreases. Less nitric oxide means less arterial relaxation, less blood delivered to erectile tissue, and less hydraulic pressure to maintain firmness. The result is erections that are less reliable, less firm, and harder to sustain.
Natural Solutions for Vascular-Related ED
L-citrulline, converted by the body to L-arginine and then to nitric oxide, has clinical evidence for supporting erectile function through improved blood vessel relaxation. Dietary nitrates from sources like beets and leafy greens support the same pathway. Cardiovascular exercise produces measurable improvements in endothelial function and nitric oxide bioavailability. For men whose vascular ED has a more significant structural component, regenerative treatments like shockwave therapy specifically target the angiogenic process, stimulating new blood vessel formation in erectile tissue to address the infrastructure problem rather than compensating for it.
Cause 2: Low Testosterone

How Declining Testosterone Disrupts the Erection Pathway
Testosterone plays multiple roles in erectile function beyond simply driving libido. It regulates nitric oxide synthase activity in penile endothelial cells, supports the health of smooth muscle in erectile tissue, maintains nerve sensitivity throughout the arousal pathway, and drives the central nervous system signals that initiate desire and arousal in the first place. When testosterone drops, all of these systems are compromised simultaneously.
What makes this particularly tricky is that testosterone decline tends to be gradual, and men adapt to the slow erosion of function without necessarily registering a clear before-and-after moment. By the time ED becomes a consistent complaint, testosterone may have been contributing to the problem for years.
Natural Solutions for Low T Contributing to ED
Resistance training involving compound movements is the most potent natural testosterone stimulus available. Sleep optimization matters enormously because the majority of daily testosterone production happens during REM sleep. Zinc, magnesium, and vitamin D are foundational to testosterone synthesis and are commonly depleted in men with symptomatic low T. Reducing abdominal fat directly reduces aromatase activity, which converts testosterone to estrogen and lowers free testosterone independently of total production. For men with confirmed testosterone deficiency, a properly supervised testosterone replacement program addresses the hormonal root of the problem where natural optimization is insufficient.
Cause 3: High Blood Pressure and Its Medications
The Double Problem: Hypertension Damages Blood Vessels and Certain Medications Make It Worse
Chronic high blood pressure damages endothelial cells throughout the vascular system, reducing nitric oxide availability and accelerating the arterial stiffening that impairs penile blood flow. This makes hypertension itself a significant independent cause of vascular ED. The medication dimension adds another layer: beta-blockers, which are among the most commonly prescribed antihypertensives, suppress sympathetic nervous system activity that is required for normal arousal and erection initiation. Thiazide diuretics increase urinary zinc excretion over time, gradually lowering testosterone as a secondary effect.
Natural solutions in this area involve optimizing blood pressure through weight management, dietary sodium reduction, regular aerobic exercise, and stress management, which can meaningfully reduce blood pressure and its vascular effects while reducing dependence on medications with higher ED risk profiles. Discussing medication alternatives with your prescribing physician is also worth pursuing, as some antihypertensive classes have meaningfully better sexual side effect profiles than others.
Cause 4: Diabetes and Insulin Resistance

How Blood Sugar Dysregulation Damages Both Vascular and Nerve Function
Diabetes affects erectile function through two distinct mechanisms that often occur together. Chronically elevated blood sugar causes glycation of vascular endothelial cells, damaging the small arteries of the penis in the same way it damages the retinal and renal microvasculature. At the same time, high blood sugar triggers nerve damage, diabetic neuropathy, which can affect the autonomic nerve pathways responsible for transmitting the arousal signal to penile smooth muscle.
The result is a combination of vascular impairment and reduced nerve sensitivity that makes ED particularly difficult to address without tackling the metabolic root cause. Even pre-diabetic insulin resistance, before frank diabetes develops, impairs endothelial function through inflammatory pathways and elevated oxidative stress.
Natural Solutions for Metabolic ED
Dietary changes that reduce postprandial blood sugar spikes, particularly reducing refined carbohydrates and processed foods, produce measurable improvements in endothelial function over weeks to months. Berberine, a botanical compound with well-documented insulin-sensitizing properties, has been shown in multiple studies to improve fasting blood sugar and reduce insulin resistance through a mechanism similar to metformin. Regular aerobic and resistance exercise improves insulin sensitivity through separate pathways. Alpha lipoic acid supports both nerve function and oxidative stress reduction relevant to diabetic neuropathy affecting sexual function.
Cause 5: Chronic Stress and Elevated Cortisol
The Stress Hormone That Shuts Down Sexual Function
Cortisol, the body’s primary stress hormone, is directly antagonistic to testosterone at the receptor level and suppresses the hypothalamic-pituitary signaling that drives testosterone production. When cortisol stays chronically elevated from psychological stress, poor sleep, blood sugar instability, or any other ongoing stressor, the hormonal environment becomes actively hostile to sexual function. The sympathetic nervous system dominance that accompanies chronic stress also directly inhibits the parasympathetic state that erections require.
Think of chronic stress as keeping your body in a state where all available resources are allocated to threat response. Sexual function is not a threat-response priority, and the body makes that allocation decision automatically. Addressing the underlying stress load through adaptogenic botanical support, sleep optimization, blood sugar stability, and structured stress reduction practices produces meaningful downstream improvements in hormonal and sexual function.
Cause 6: Sleep Deprivation and Poor Sleep Quality
Why Your Body Runs Testosterone Production During Sleep
The majority of a man’s daily testosterone production happens during deep, slow-wave and REM sleep, with a distinct overnight surge that produces the morning testosterone peak and the morning erections that are a useful clinical indicator of intact erectile physiology. Chronic sleep deprivation or poor sleep quality from sleep apnea, pain, or poor sleep hygiene interrupts this production window and drives cortisol upward simultaneously, creating a dual hormonal suppression effect on sexual function.
Men with obstructive sleep apnea have significantly higher rates of ED than the general population, even when controlling for age and other risk factors, because repeated nighttime hypoxemia and sleep fragmentation both suppress testosterone production and impair vascular endothelial function. Addressing sleep apnea through CPAP therapy or weight-related improvements often produces meaningful improvements in erectile function independently of any other intervention.
Cause 7: Medications Beyond Blood Pressure Drugs
Antidepressants, Antihistamines, and Other Prescription Culprits
SSRIs and SNRIs, the most commonly prescribed antidepressant classes, produce sexual side effects including reduced libido, delayed ejaculation, and impaired erectile function in a substantial percentage of users. The mechanism involves their effects on serotonin signaling, which modulates dopamine, a key driver of sexual desire and arousal. Antihistamines with anticholinergic activity, certain antifungals, 5-alpha reductase inhibitors used for hair loss or prostate health, and opioid medications all have documented effects on sexual function through various hormonal and neurological pathways.
Having the Medication Conversation With Your Provider
This is one of the most important and underutilized conversations in men’s health. Many men have been on medications for years without anyone connecting them to changes in sexual function that developed after starting those medications. Bringing a complete medication and supplement list to an integrative provider who will systematically evaluate each item for sexual health effects can reveal contributors that have gone unnoticed for years and open discussions about alternatives, dose adjustments, or complementary approaches that mitigate sexual side effects.
Cause 8: Obesity and Metabolic Dysfunction
How Excess Adipose Tissue Creates a Hormonal and Vascular Crisis
Abdominal adipose tissue is metabolically active in a way that directly suppresses male sexual function. It contains high concentrations of aromatase, the enzyme that converts testosterone into estrogen. Men carrying significant excess abdominal fat commonly have low free testosterone and elevated estradiol regardless of their testosterone production, because the conversion is happening faster than production can keep up. Elevated estradiol then further suppresses hypothalamic testosterone signaling through negative feedback, compounding the deficit.
Beyond the hormonal impact, obesity drives chronic low-grade systemic inflammation, insulin resistance, and dyslipidemia, each of which independently damages endothelial function and reduces nitric oxide availability in the vascular system that supports erection. Addressing obesity is not a cosmetic issue in the context of ED. It is a direct intervention on multiple causal pathways simultaneously.
Cause 9: Pelvic Floor Dysfunction
The Structural Issue Most ED Discussions Skip Entirely
Pelvic floor muscles play a direct mechanical role in erectile function, supporting the veins that maintain pressure in erectile tissue during erection. Hypertonic or overactive pelvic floor muscles, which can develop from chronic pelvic tension, prolonged sitting, prior trauma, or prostatitis, restrict blood flow dynamics in erectile tissue and impair the veno-occlusive mechanism needed to maintain erection. Paradoxically, overly lax pelvic floor muscles from deconditioning can produce the same result through inadequate venous support.
Pelvic floor physiotherapy, targeting the specific dysfunction identified through assessment, produces measurable improvements in erectile function in men with this structural contributor. It remains one of the most underutilized and underrecognized interventions in the ED treatment landscape, largely because it requires specialist assessment to identify and is rarely included in standard ED evaluations.
Cause 10: Psychological Factors and Performance Anxiety
When the Problem Starts in the Mind and Becomes Physical
Psychological causes of ED, including performance anxiety, depression, relationship stress, and unprocessed trauma, are particularly common in younger men and in men whose ED developed after a specific triggering event. The parasympathetic nervous state required for erection is directly suppressed by anxiety, which activates the sympathetic system. A single episode of erectile difficulty from any cause, even a temporary physical factor like alcohol or fatigue, can trigger performance anxiety that then perpetuates the problem independently of whatever originally caused it.
Breaking the Anxiety and ED Feedback Loop
The anxiety and ED loop is self-reinforcing by design. The more a man anticipates difficulty, the more sympathetic activation he brings to sexual situations, and the more likely the anticipated difficulty becomes. Breaking this loop requires both addressing whatever physical contributors may be present and working with the psychological dimension directly, through cognitive behavioral approaches, mindfulness-based practices, or in more significant cases, working with a therapist experienced in sexual health. Addressing the physical contributors through proper evaluation often provides the psychological relief needed to interrupt the anxiety loop as well.
Getting a Proper Evaluation Instead of Guessing
The most important insight across all 10 of these causes is that guessing which one applies to you is not a strategy. Many men present with two, three, or more contributing factors operating simultaneously, and addressing only one while leaving others unexamined produces incomplete results. A thorough evaluation at a clinic specializing in men’s sexual health covers hormonal status, cardiovascular risk markers, metabolic function, medication review, sleep quality, and psychological history together.
At Proactive Choice, men seeking care for erectile dysfunction receive exactly this kind of comprehensive assessment. Understanding which of the 10 causes of erectile dysfunction applies to your situation is what makes it possible to build a treatment plan that actually addresses the real problem rather than covering for it. For men in Bend looking for genuine answers, working with an experienced men’s health clinic that takes this whole-picture approach changes the trajectory of care entirely.
The most effective ED treatment is one matched to the actual cause. Whether that involves optimizing testosterone levels, supporting vascular health, addressing sleep, reviewing medications, or a combination of approaches, ED treatment Bend at Proactive Choice is built around finding and addressing what is actually driving the problem in your specific case. For men whose evaluation points to a significant hormonal component, a proper assessment of testosterone levels and replacement options is often the starting point that changes everything else.
A Note on How This Article Was Created
This article was written to give men dealing with erectile dysfunction a clear, thorough understanding of the most common root causes and what natural solutions align with each. The clinical perspectives throughout reflect Dr. Drew Collins’ direct patient care experience across more than four decades of integrative men’s health practice. This content is educational and does not substitute for an individualized medical evaluation. A direct consultation with Dr. Collins or another qualified provider is the appropriate next step for guidance specific to your situation.
Conclusion
Erectile dysfunction is almost never one single thing. It is a signal from the body that one or more systems involved in sexual function are not working as they should, and the most useful response to that signal is investigation rather than symptom suppression. Whether your ED has a vascular root, a hormonal driver, a medication contributor, a sleep problem underneath it, or some combination of several factors working together, identifying the actual cause is what makes treatment genuinely effective rather than temporarily compensating for an unresolved problem.
Men who get a thorough evaluation and address the real contributors to their ED consistently report better outcomes than those who cycle through generic treatments without understanding what they are actually treating. That deeper understanding, and the personalized care that follows from it, is what makes the difference between managing a problem and actually resolving it.
Frequently Asked Questions
How do I know which of these 10 causes applies to me without seeing a doctor?
You probably cannot know with confidence, and that is actually the most important point. Many men have two or three contributing factors operating simultaneously, and self-diagnosing based on symptoms alone leads to addressing the most obvious cause while missing others. A proper hormonal panel, cardiovascular risk assessment, medication review, and thorough health history taken together give you actionable answers. The evaluation itself is where the real value lives, not in the guesswork that precedes it.
Can natural solutions for ED work as well as medications like Viagra or Cialis?
For mild to moderate ED with identifiable root causes, addressing those causes naturally can produce results that are more sustainable than medication alone because they improve the underlying function rather than temporarily compensating for it. Medications like PDE5 inhibitors work by enhancing a mechanism that is already present, which means they work best when that mechanism is only partially impaired. When the underlying vascular, hormonal, or metabolic causes are addressed alongside or instead of medications, many men find their erectile function improves in a way that feels more reliable and does not require pre-planning around a pill schedule.
At what age does ED typically start and is it inevitable?
ED becomes more common with age, but it is not an inevitable part of aging when the underlying contributors are addressed. The increased prevalence in older men reflects the accumulated cardiovascular, hormonal, and metabolic changes that develop over decades of lifestyle and health history, not age itself as a fixed cause. Men in their 60s and 70s who maintain good metabolic health, healthy hormone levels, and cardiovascular fitness typically have meaningfully better erectile function than those who do not, regardless of age.
If stress is contributing to my ED, does that mean it is all in my head?
No, and this framing causes real harm. Psychological and physiological causes of ED are not opposites. Chronic stress produces measurable changes in cortisol levels, testosterone suppression, and sympathetic nervous system activity that are just as physiologically real as arterial plaque. Performance anxiety produces genuine neurological and vascular effects that impair erectile function through concrete biological mechanisms. Saying ED from stress or anxiety is all in the head misunderstands how the mind and body actually communicate, and it often prevents men from getting the help they need.
What is the first test I should ask for if I think I have ED?
A morning total and free testosterone draw is often the highest-yield starting point because low testosterone is both common and frequently missed by providers who only check total testosterone without free testosterone and SHBG. A fasting metabolic panel including fasting glucose and insulin reveals insulin resistance that is frequently undiagnosed. A full lipid panel, complete blood count, and inflammatory markers round out a basic cardiovascular and metabolic picture. If sleep problems are also present, a sleep apnea screening is warranted. Bringing a complete medication list to your first appointment gives your provider the opportunity to identify pharmaceutical contributors that are often overlooked.